As the State of California invests billions to expand Substance Use Disorder (SUD) treatment facilities, a state grant ($11 million for just one), to fund construction of two new treatment facilities in a rural residential neighborhood in Rescue, California, has sparked a contentious debate. At the heart of this controversy is a fundamental question: Why choose sites that jeopardize safety and are at odds with the well-being of those they seemingly aim to serve?
This editorial delves into the perplexing choice of these ill-advised locations for these proposed SUD facilities, and how they will undermine the recovery process, strain the fabric of the existing communities and significantly increase safety risks to all involved. As we unravel the layers of this proposal, we must also confront the unsettling echoes of history and the potential repercussions on vulnerable populations seeking a path to healing.
We assume you, the reader, already have a basic understanding of the situation Rescue Deer Valley is fighting. This editorial is not meant to be a comprehensive review of all the issues pertaining to these proposed developments, but rather to help our community try to understand why the choice of the Deer Valley Court parcels in Rescue for these two facilities should be opposed. If you want background information, be sure to review the information in this website, or you can also read the FAQ (link) to get quickly up to speed.
Rescue, CA- a poor location for these new SUD facilities
Since the first moment our community found out about these ill-advised proposals we have asked “Why Here, this doesn’t make any sense?” Why would a business want to build two large commercial facilities, housing up to 80 people a day, in a rural residential community of single-family homes? As we learned more about the population that these facilities are meant to serve, it became even more puzzling. According to news releases and the grant application, the target population is “predominantly” from San Joaquin County, but actually can come from “anywhere in California.” How does constructing SUD facilities far away from marginalized communities and transporting patients from anywhere in California make sense? It makes sense for profit, but not for the clients.
The Rescue locations/parcels are located in the Highest Severity Fire Risk zone in California (link) and are miles away from any major road access. This concentration of people in this High Severity Fire Risk area is counter to the Governor’s Office of Planning and Research and is in direct conflict with the State Fire Code (CCR 1273-1273.9) related to ingress and egress during a wildland fire. As a practical matter, every trip to/from these buildings by staff or patients must traverse a dangerous, narrow road, with single and narrow lane bridges to get to anything. The nearest medical facilities are 10 miles away, taking approximately 20 minutes one way (according to Google Maps). Emergency services are delayed due to the location and road access. So why here?
While the developer, HomeCA (link), has offered statements about the peaceful nature of these locations and the “native communities we aim to serve”, they do not offer a rational explanation of why they want to build far away from the locations of the native communities they are serving and require them to relocate for services. Amazingly, in the state grant application, they acknowledge these communities do not have local services, so instead of addressing that problem, they offer transportation to these far away locations. How did this get through the review process?
The managing care provider, Native Directions Inc (NDI)(link), could have worked with, and still can work with, HomeCA to choose anywhere in California for these facilities. NDI has operated an 18 and over Native American male substance use disorder (SUD) facility in Manteca for decades. They must know the county and first responders well. Certainly, they could have found parcels offering a peaceful setting in their local county that would be much safer and have much better access to services and be closer to transportation hubs as they expanded their facilities to support female patients. What drove them to these unsuitable far away parcels in Rescue?
Displacing Native American patients from their families
How does the proposed plan of transporting these marginalized, pregnant women, and their children, far away from their families and any support systems help them overcome their issues long term? These treatments are temporary (90-120 days) and these patients, and their children, will most likely be transported back to their current residences once they complete their treatment, although that is not clear. If their children are of school age, they will need to be placed, temporarily, into a brand-new school situation, and then uprooted once again once the treatment is completed. If they are not transported back or they leave the facility before completing treatment, they will be in an area with no services for them. Loving family members will not be able to participate or support this treatment in person as they likely will be unable to travel the long distances to Rescue to stay in touch with the patients and their young children. Yes, even people vulnerable to or experiencing homelessness have families who care and are desperate for their loved ones to get the help they need. There are no hotels or services nearby, further discouraging visits. Is that really in the best interest of the people being treated? This approach lacks the necessary continuum of care and long-term support essential for sustainable recovery.
The United States Government has a poor history of “transporting” Native American people “for their benefit.” Some in our Rescue Deer Valley community have Native American heritage, and their families have experienced displacement. They are truly concerned that native Americans are again being treated differently, and for the well-being of these future patients and their children as this proposed facility uproots them from loved ones and any support network and sends them far away, to these unsuitable Rescue locations. Shouldn’t these treatment centers be built in peaceful and safe locations closer to where the patients currently live?
Ignoring State Priority – Geographic Equity
The state programs that plan to fund these developments are meant to expand and fill gaps in local support infrastructure in disenfranchised communities, including mental health and SUD treatment and continued care facilities across California. Governor Newsom has said “housing is number one.” One of the top priorities of the Department of Health and Human Services is achieving Governor Newsom’s goal through “Geographic Equity,” as they emphasize in their letter to the EDC Board of Supervisors (link).
This same priority is listed in the following Behavioral Health Continuum Program (BHCIP) program update (link) – which states: “A gap analysis on BHCIP funding to-date coupled with existing behavioral health facilities across California has shown several regions, along with tribal entities, that continue to display unmet needs. Many counties in these regions are rural and/or small, making it challenging for individuals in these communities to readily access needed behavioral health services.”
With the stated priority of Geographic Equity above, and the following point made on ensuring investment goes to communities that need ready access to behavioral health services, why would DHCS transport pregnant women 100’s of miles away from their families, friends and established medical providers for Substance Use Disorder (SUD) treatment? This certainly does not fill a gap in needed services within disenfranchised communities, nor does it expand the continuum of care. In fact, this plan to centralize treatment far away from these communities will actually hinder geographical equity with competing interests for projects that would expand and fill that gap in geographical areas of need.
These locations in Rescue, for patients “in the San Joaquin Delta area” (link) or anywhere in California, does not put the facilities into communities that need more of these services. The unfortunate future patients of these facilities will need to be transported far away from home and any existing medical care to a treatment center that has no services, is far away from medical care, and is in the highest fire risk in the state. This is costly and provides an advantage only for profitability.
El Dorado County Already Serving Native Population
We met with individuals in the El Dorado County (EDC) Health and Human Services Agency to ascertain the need for Native American Perinatal and Bridge Housing facilities in this county. While EDC certainly has areas of investment needed for county behavioral health, EDC has a very active Native American tribe, the Shingle Springs Band of Miwok Indians, that has invested in significant behavioral and physical health infrastructure for Native American county residents. As noted by Congressman McClintock, this group opposes the proposed locations of these facilities (link). Wouldn’t Native Americans located in San Joaquin County appreciate the investment in long-term infrastructure and benefits of additional facilities in their county?
Also consider the community value of these State investments. As DHCS stated above, there are regions that have “unmet needs” for behavioral care facilities, and in this case Native American tribal facilities. El Dorado County is not a participating county in the program funding these facilities (link). San Joaquin County, which is the county where Native Directions has decades of experience, is a participating county, so we must presume they have unmet needs. Why isn’t this $11 million facility being built in a county that has identified needs, and is closer to the population being served? Even better, why not use that $11 million to expand upon or build several smaller facilities within several different areas of need, that would offer continued care after treatment? Stated another way, the current plan spends $11 million on one treatment facility, in an area where it is not needed, and not $1 dollar goes to build or expand in local areas of need.
Failure to coordinate with the local county/community
While the state program specifically states that the applicant is to coordinate with the local county, community, and tribal council, Home CA never did. The first Deer Valley Court parcel HomeCA purchased was in April, 2022. As Rescue Deer Valley learned about these proposed facilities and started engaging with our county officials in December, 2023, 18 months later, this was the first they had heard of these proposed facilities (link). HomeCA has not answered any of the community inquiries regarding their plans. As of June 2024, to our knowledge, they still had not met with county officials, except through their contractor permit applications. They have worked hard to keep the community in the dark. What are they trying to hide?
Inflated Land Values to Receive More Grant Funding
HomeCA has presented to the State much higher appraisals than their purchase prices of the properties as the basis used as collateral in these state grant proposals. As these real estate investments are the basis for the size of grant monies HomeCA can be awarded, the higher the appraised value, the higher the grant they can receive.
The property at 3335 Deer Valley Ct was purchased by Gina Wasdyke/HomeCA for $260K in May 2022, with an assessed 2023 value of $266K. This property has been offered for sale over many previous years without being sold until this sale to Gina Waskyke/HomeCA. It is a challenging parcel to develop on as half of the acreage is on a steep hill and covered in granite bedrock. It also is in the Highest Severity Fire Zone, as noted in the Cal-Fire Severity Zone map of California (link). It is only accessible via dirt roads and residents must traverse Deer Valley Road (link) to get to any stores or services, so it is not a location for individuals that will be making multiple trips per day to external parties. This purchase was made in a declining real estate market, as interest rates had gone up significantly – see table below.
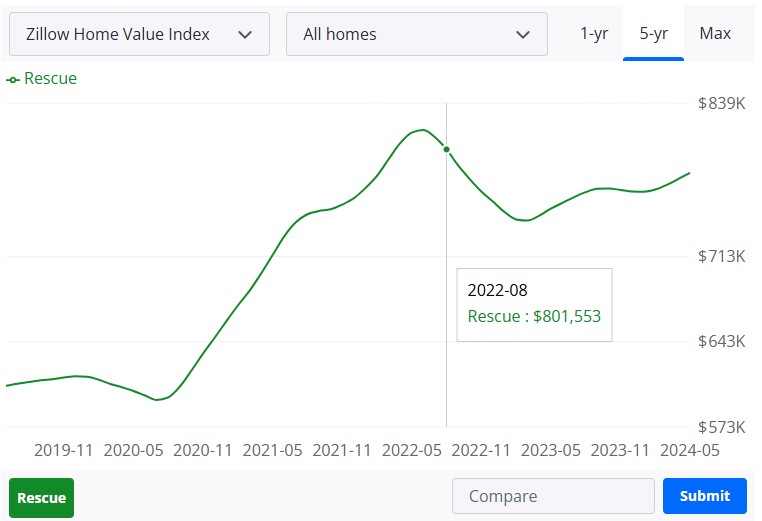
Purchased 05/22, Appraised 8/22 in a declining market
After owning this property, a little over a year, with no improvements made, and in an overall market that was significantly down, HomeCA demonstrated to the State a “certified” appraisal of $435K on their 8/29/22 grant application, claiming an appreciation of $199,000 in value. What was the basis for the significant increase in property value with no improvements made and during a declining overall real estate market?
Grant Application for 3335 Deer Valley Ct Facility – Certified Appraisal $435K

Poor Patient Experience
These facilities are proposed for a rural residential neighborhood in Rescue, accessible only via one main road, with no walking/biking trails or close proximity to any retail establishments. Patients going through treatment will have nothing available to them within walking distance of the facility and will need to be transported for any external need. With up to 70 patients combined across the two facilities, transportation services will likely have spotty availability for the patients. All trips to/from the proposed facility need to traverse Deer Valley Road, which is a narrow, twisty road with blind corners and single lane bridges. There are many blind corners where traffic would not have visibility to any pedestrian traffic (link).
One of these facilities is designed to serve pregnant women during, and just after, their pregnancy. These patients will be receiving therapy and treatment onsite for their substance use disorder, while also dealing with their pregnancy and childbirth. They will need to routinely be transported to/from medical services during these critical months. This road, along with the rural location, slows down emergency response as well. Recent resident experience has been 20 minutes for police response, although local fire response has been quicker. A hypothetical 911 medical emergency estimates 40 minutes, best case, from the call to the closest hospital (link).
As noted above, these facilities are proposed to be built in the most severe fire danger zone in California – Very High Severity wildfire risk zone. Patients and staff will need to be very careful if they want to smoke or use fire for any reason as these parcels are surrounded by unmaintained bushy areas. There is only one access road in/out of this residential area. In the event of an emergency wildfire evacuation and response, the added number and concentration of people associated with these facilities would block evacuation and response routes. These facilities are designed to house 70-80 people, including disabled and children, all attempting to board 10 vans at once, or multiple van trips over a period of time, all while first responders are trying to gain access to the area, along with the evacuation of those in single family homes. As previously stated, this violates State Fire Code of Regulations Section 1273.
A wildfire took place in this area in 2002 and it was a problem then. The proposal to build high density commercial facilities in this area is reckless. Clearly, the developer failed to conduct due diligence. When a wildfire occurs, a question will be asked- Why were these facilities built when governing officials knew about the dangers before they were built?
Conclusion
To summarize, these two proposed facilities in Rescue, CA need to be stopped and the grant money diverted to facilities closer to the populations they are meant to serve, and in geographic locations that need additional infrastructure investment. Displacing Native American women from all around California and transporting them to these parcels in Rescue are a disservice to them and place them in additional hardships due to the nature of these locations. El Dorado County, and the Miwok Tribe of Shingle Springs Indians, have already created infrastructure to serve the local needs of El Dorado County, so the state needs to guide these new investments into more deserving locations, and on parcels better suited to the needs of the patients, rather than the convenience of the developer.
In conclusion, the proposals for the Native American Perinatal and Bridge Housing facilities in Rescue are in an unsafe location and fundamentally flawed. These facilities, intended to serve vulnerable populations, are being placed far from the communities that need them most, contradicting the state’s priority of Geographic Equity. The decision appears to be driven more by financial gain than by the well-being of the patients. It is imperative that these facilities be relocated to areas where they can truly benefit the intended populations, ensuring that investments in behavioral health services are both effective and equitable. The voices of the Native American communities and the principles of fair access to care must guide these critical decisions.
We need your help. Please subscribe to our website to receive regular blog post updates by clicking here, that way you can be informed on latest activity, as well as providing support and input. If you want to add your voice please contact the State Directors that control these budget dispersals. You can find their contact information here.
Published July 10, 2024
